Submitted by Benjamin’s mother, Selena
The Homebirth of Benjamin David, 15th March 2012

After the beautiful natural birth of my first baby, and then an awesome planned vaginal breech for my second, having a homebirth for my third was a no-brainer. I trust my body and knew that I needed to be in a comfortable, private, sacred space where my hormones could do their job undisturbed, so what better place than at home? I announced my plans to homebirth and even ‘pre- booked’ my midwife (Lisa Richards) before I was pregnant, I just couldn’t wait! I love giving birth, and as it was going to be my last baby I wanted it to be nothing short of perfect.
The pregnancy was easy and enjoyable. It was such a treat to stay home for all my antenatal appointments, which felt more like social catch-ups with a good friend. I organised for two other friends to attend the birth: Jane to take photos and Kate to be with my girls, aged 5 & 2, who we hoped would have the amazing experience of seeing their little brother or sister being born. The fact that both women also happen to be midwives was reassuring, even though I had total confidence in Lisa.
Because both my girls arrived at 39 weeks, I assumed that this Bub would follow suit, and I predicted (and announced to anyone who asked) that s/he would probably be born on the auspicious date of Feb 29. My EDD was March 7. From 38 weeks I started telling Lisa at each weekly visit that we didn’t need to make another appointment because I was so sure I’d be giving birth before then. And then the week would pass without event and I would greet her at our next appointment feeling a little deflated. I couldn’t understand why it wasn’t happening when I was so ready and so excited! I’d had a blessingway and a pregnancy photo-shoot, road-tested the birth pool, chosen music & aromatherapy oils, designed a mud-map of my birth space, painted a trust mandala onto canvas… even my stainless steel mixing bowl with plastic bag liner was ready and waiting on our loungeroom floor to catch a placenta. The bassinet was set up in our bedroom… but something was wrong. For some reason and try as I might, I couldn’t visualise a baby in it. I couldn’t even visualise myself in labour… it all felt so far off, despite the fact that I was ‘due’ and wanted it so badly. So what was I doing wrong? Why didn’t my baby want to be born?

It wasn’t a good headspace to be in, and knowing how powerful the mind is, I realised I had to let go of certain anxieties that I suspected were holding things up. I was finding it difficult to accept that some things weren’t happening according to plan. My Mum had come to stay, but she was supposed to arrive after the baby was born, not before, because even though I love her lots, I preferred not to have her in my birth space. And now that she was here I had to face that probability, and also tell Kate that I didn’t need her anymore, which was disappointing. I wasn’t used to being ‘overdue’, and because of my Feb 29 prediction everyone thought I was a week further along than I actually was, so I was feeling pressured and increasingly annoyed by all the comments I was receiving… “You still here?!”, “Hasn’t the baby arrived yet??!!”, “Is it safe to homebirth when you’re overdue?”, “When are you going to get induced?” etc. I’d lost my sense of excitement to a certain degree as Braxton Hicks kept amounting to nothing & the comments kept coming, and I started to wonder if Bubby was ever going to arrive. I’d also wanted to have lots of R&R time to meditate and connect with the baby in the lead up to the birth, but aside from one yoga class per week this wasn’t happening either. My husband David was working lots so I was still as busy as ever doing everything for the girls and the running of our household… needless to say I was feeling very frazzled!!!
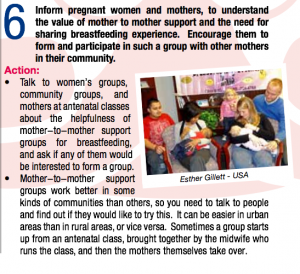
So I made a momentous decision at my 41 week appointment on March 14. “Face of Birth” was screening locally that night, which I hadn’t been planning to attend (I’d already bought tickets to the next screening instead), but I decided that it was probably just the thing I needed… so I told Lisa I’d join her there. We joked that I would probably give birth in the theatre amongst my ‘village’ of like- minded women, and I felt my excitement returning as I gave myself a little stretch & sweep in the shower before heading out.
So many moments in the film really hit home for me and confirmed everything that I know to be true about birth. When the Aboriginal woman declared that “we are holy women when we give birth”, I had tears streaming down my face as I recalled telling David, my Mum & Lisa that my birth space was sacred – quiet, respectful & candlelit, where anyone present would behave as though in church or in the company of a higher presence. The film undoubtedly reconnected me with my birthing ‘mojo’ and inspired me to let go of everything that was weighing me down, and just let this birth unfold however it was meant to. I was back in tune with my baby and my instincts, and when I said goodbye to Lisa I knew I’d be seeing her again very soon…
I got home at 10:30pm and was in bed by 11pm listening to my Calmbirth CD, visualising the birth with lots more clarity now, when at 11:30pm Bubby kicked so hard that I felt an odd pop, realising soon after that I was very wet. I lay there quietly for several minutes in surreal disbelief, wondering what it was… urine, blood, semen, amniotic fluid?? Could it be??!!! I began to feel some regular tightenings so I tottered off to the bathroom, where I discovered that my membranes had indeed ruptured, and by midnight contractions were established and 10 mins apart. I let Lisa & Jane know and went back to bed full of delicious anticipation (like it was the night before Christmas!) whilst David quietly got to work setting up my birth space in the loungeroom. When I made my way out there an hour or so later I was blown away – it was bathed in candlelight with music & aromatherapy oils softly spilling into the room, the ‘purple pool’ full & inviting… such a warm, comfortable, sacred space, exactly as I had imagined! Mum and the girls slept soundly nearby in their beds – it couldn’t be more perfect.
I spent the next hour quietly breathing through the waves as I leaned over the lounge (kneeling on the floor), while David gave me a beautiful back massage. Sometime after 2am things had ramped up a gear, so despite feeling bad about waking Lisa & Jane, I texted them to let them know that they should probably come. Little did I know that ‘ramping up a gear’ was actually ‘transitioning’! Luckily Lisa lived only 10 minutes away because when she arrived I was in second stage, realising with some regret that I wasn’t going to make it into the pool – Bubby wasn’t far away! I was on my yoga mat leaning over my fitball now, rolling back and forth with each wave, feeling Bubby descend and my body open up whilst I was instinctively bearing down at the tail end of each exhalation… such an incredible sensation! I remember thinking that if Mum was awake and hearing my orgasmic “aaaaah”s, she would think David & I were makin’ whoopee in the loungeroom! It was definitely pleasure as opposed to pain.

Lisa wasn’t there long before I asked her to take my undies off – she hadn’t realised things had progressed so far and was surprised to see a head crowning. I reached down and felt it as David got into catching position, and after a couple of pushy exhalations through a ring of friendly fire, a little head was gently born… and then our precious Benjamin David slid beautifully into his Daddy’s hands at 3:09am. A boy!!! And in only three hours! David passed him back through my legs to me, and we had a lovely group hug, marveling at our perfect little man, before I moved onto the couch to get comfy for a nice long skin-to-skin breastfeed. After an hour or so I felt the need to sit up and realised that I was also feeling a bit ‘pushy’ again… my body was doing its job beautifully, and within minutes I birthed my placenta into the bowl and lay back down again. It sat beside us for another hour or so, still connected to Benjamin, until the cord had long-stopped pulsating and David cut it.
We all sipped champagne by candlelight and marveled at the whole experience, all high on oxytocin, until daybreak when Mum and the girls woke to meet our gorgeous new family member… none of them realising that he was being born as they slept! It was so surreal and SOOOO sublime. And I felt like a goddess.
Lisa was amazing. She cleaned everything up so quickly & efficiently and stayed with us well into the morning to give me a shower and tuck me into bed – such attentive TLC that one couldn’t possibly receive in hospital. Jane took some incredible photos. I hardly knew she was there as she captured all the miraculous moments that are etched in my memory forever. And my Mum was great too, feeding us all toasted hot cross buns and opening her arms for my girls as they slowly took in the surprise of waking up to a new little brother. She took care of them so David and I could snuggle up in bed together with Benjamin, which is where we remained cocooned all day, drinking him in.
The whole experience surpassed all my expectations in the end, and it taught me some valuable lessons… that too many expectations can result in too much anxiety; and that I needed to quiet my mind and let go of these expectations, and simply let the birth unfold in its own time and find its own perfection.
Thank you Selena and family, and Jane McCrae for sharing!
Readers, please consider sharing Your Birth Story with the O Birth Pod Cast. Join us Tuesday Nov 26 (with access all week) for eClass w/ Sex Coach Kim Anami.