7 June, 2014
Parents, grandparents, aunts, uncles, siblings, families, midwives, doulas, doctors, nurses, hospital administrators and legislators… we are BirthKeepers. It is our responsibility to ask the next and the next question, for as BirthKeepers, it is we who are given the sacred responsibility to protect our incoming humans, the newborns, at birth and as they grow, for they are the future EarthKeepers. My question now is: “Are we allowing our health providers to rob our babies, of their full potential of health, intelligence, immunity and longevity, at birth?”
According to the Red Cross, children under the age of 17 (16 with parental consent in some States) are not eligible to donate blood. Blood donations are generally no more than 1 pint, which is 1/10th of the average adult blood volume. Blood donors must weigh at least 110 lbs (49,895 kg).
Yet, all over the world, in nearly every single medical institution where babies are born, Newborn infants (usually weighing only between 2 and 5 kilograms) are being denied up to 1/3 of their blood volume.
At the moment of birth newborn infants are estimated to have a blood volume of 78 ml/kg (X 3.5kg = 273 ml) with a venous hematocrit of 48%.
When the umbilical cord-clamping was delayed for 5 minutes the blood volume increased by 61% to 126 ml/kg (X 3.5 kg or 7.7 lbs. = 441 ml). This placental transfusion amounted to 168 ml for an average 3,500 g infant, one-quarter of which occurred in the first 15 seconds, and one-half within 60 seconds of birth.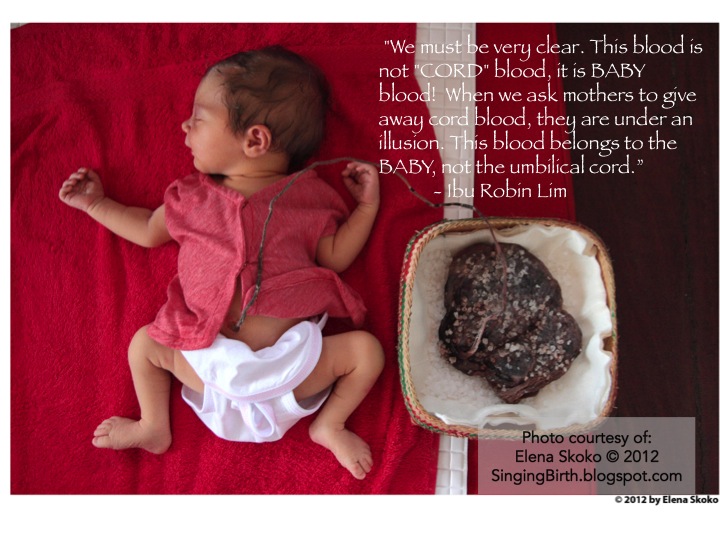 Is taking 1/3 of a mammal’s blood supply harmful? How then can it be legal, for hospital protocols and practices to harm newborns, by robbing them at birth, of so much of their blood? I have reviewed the research and the evidence, and found absolutely NO benefits for newborn babies, when their umbilical cords are immediately clamped and cut at the time of birth. In fact the studies prove this to be a harmful practice. I am quite sure that if I went removed 1/3 of even one adult patient’s blood, without his or her consent, it would be considered a crime. There would be media outcry against me, and I would be prosecuted. How then is it that people tolerate the same unfair treatment of human neonates?
Is taking 1/3 of a mammal’s blood supply harmful? How then can it be legal, for hospital protocols and practices to harm newborns, by robbing them at birth, of so much of their blood? I have reviewed the research and the evidence, and found absolutely NO benefits for newborn babies, when their umbilical cords are immediately clamped and cut at the time of birth. In fact the studies prove this to be a harmful practice. I am quite sure that if I went removed 1/3 of even one adult patient’s blood, without his or her consent, it would be considered a crime. There would be media outcry against me, and I would be prosecuted. How then is it that people tolerate the same unfair treatment of human neonates?
 A mountain of research does point to the fact that by simply delaying the clamping and cutting of babies’ umbilical cords, our newborn children would suffer less trauma, fewer inner cranial hemorrhages, have higher stores of iron at 4 months of age, and even up to 6 and 8 months after birth. , , The nutrients, oxygen and stem cells present in the blood transfused into babies by the placenta, when cord severance is delayed ensures the bodies’ tissues and organs are properly vitalized, supplied with energy, and nourished. This translates into improved health, heightened immunity, more intelligence and perhaps, potential for increased longevity.
A mountain of research does point to the fact that by simply delaying the clamping and cutting of babies’ umbilical cords, our newborn children would suffer less trauma, fewer inner cranial hemorrhages, have higher stores of iron at 4 months of age, and even up to 6 and 8 months after birth. , , The nutrients, oxygen and stem cells present in the blood transfused into babies by the placenta, when cord severance is delayed ensures the bodies’ tissues and organs are properly vitalized, supplied with energy, and nourished. This translates into improved health, heightened immunity, more intelligence and perhaps, potential for increased longevity.
In addition, by not severing the umbilical cord at birth, the baby must stay skin to skin with mother. This eliminates or greatly reduces the potential for birth trauma. Research has proven that babies born without trauma enjoy an intact capacity to love and trust. (Michel Odent OBGYN “The Scientification of Love.)
The simple, natural, common-sense practice of giving the placenta time to do its job, of delivering to the baby, his or her full blood supply, has been criticized and NOT implemented by the very doctors and hospitals who have taken an oath, to “Never Do Harm.”
An intervention, by definition is an action or process of intervening, or interfering, and so, the clamping and cutting of human babies’ umbilical cords is an intervention. However, in the medical literature, I have repeatedly seen the delay of umbilical cord severance called, an “intervention.”
Surgery is an intervention, in some cases a life saving one. I wonder, how not interfering with a natural, healthy process may be deemed an intervention. The imposed medical habit of immediately clamping and cutting babies’ umbilical cords has not been with us so long (just over 200 years) and yet, it is considered “normal” and “necessary.”
“Another thing very injurious to the child, is the tying and cutting of the navel string too soon; which should always be left till the child has not only repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much weaker than it ought to be, a portion of the blood being left in the placenta, which ought to have been in the child.” Erasmus Darwin, Zoonomia, 1801
The habitual practice of immediate umbilical cord clamping and cutting began in the 1960s when a hypothesis arose among physicians thinking that immediate cord severance would prevent jaundice. If this was true why do so many babies who had their cords immediately clamped and cut, need phototherapy for pathological jaundice? Research has proven that there is no greater risk of pathological jaundice for newborns whose cord clamping and cutting was delayed.
Another theory was that early cord clamping would prevent Polycythemia, or too much hemoglobin. Some research does show an increased concentration of hemoglobin in the delayed cord clamping group, but it has not harmed babies, nor is it a significant argument for immediate cord severance.
When immediate umbilical cord clamping and cutting was introduced, it was never questioned. NO research was conducted to determine if it was a safe practice. It was just done for convenience. Doctors, nurses and midwives began to follow the trend, like sheep wearing blinders. Later, they justified it with myths about delayed cord severance causing jaundice. Few asked the questions I am asking today; “What about the Baby?” “What are the Babies’ human rights?” “Is the practice and protocol of immediate umbilical severance harming our children?” “Is it sabotaging breastfeeding and bonding?” “Is it impairing our children’s birthright to their full potential of health and intelligence?” At this junction on herstory and history, many BirthKeepers are asking these very questions.
The research proves that immediate or early umbilical cord severance is detrimental to our newborn children, but no one seems alarmed? Are we hypnotized? Why are we trusting medical professionals, who profit from denying our offspring their very blood?
Thinking, caring parents and grandparents have concluded that OBGYNs and midwives, who insist on habitually severing the umbilical cords of newborn babies, immediately, are simply protecting their right to practice with impatience, and what they deem ‘efficiency,’ with no regard for the rights of the baby, who cannot protest.
Due to imagined Fear of litigation. In 1995 the American Academy of Obstetricians and Gynecologists (ACOG) released an Educational Bulletin (#216) recommending immediate cord clamping in order to obtain cord blood for blood gas studies in case of a future lawsuit. They did this because deviations in blood gas values at birth can reflect asphyxia, or lack of. Lack of asphyxia at birth is viewed as proof in a court of law that a baby was healthy at birth.
Following an unpublished letter sent to ACOG by Dr. Morley, ACOG withdrew this Educational Bulletin in the February 2002 issue of Obstetrics and Gynecology, the ACOG journal. This action released them of liability resulting from their previous bulletin #216 of 1995. Parents and all BirthKeepers must ask; WHY, if ACOG has withdrawn its erroneous instruction to doctors, to immediately clamp and cut babies’ umbilical cords, is it still universally and dangerously practiced? Midwives and doctors who propose to preserve the healthy process of placental transfusion at birth, by delaying umbilical cord clamping and cutting, are criticized and charged with the burden of proving that letting nature take her course is, safe!
At Bumi Sehat we have received nearly 7,000 babies safely into the world, in high-risk, low resource settings. ALL of them enjoyed delayed umbilical cord clamping and cutting. Normally we wait 3 hours before doing anything with the Babies’ umbilical cords, and many parents choose cord non-severance, or, “Full Lotus Birth.” My grandsons, had what is called, “Full Lotus Birth” their placentas were left intact. Full Lotus Birth is simply allowing the baby, umbilical cord and placenta to stay intact, until the cord naturally dries and falls away, with no violence. Partial Lotus Birth happens anytime we see the baby, cord and placenta trinity. This means we do not clamp or cut the babies’ umbilical cords, before the placenta has been safely born. Certainly we would never clamp and cut a baby’s cord, until all pulsation has stopped.
At Bumi Sehat we have experienced NO ill effects for the babies, even though we do not immediately sever their umbilical connection to the placenta. A small study was done which compared a small sample of 30 babies from Bumi Sehat (greatly delayed cord severance) and 30 babies from a local hospital with immediate cord severance. There was NO increased rate of Jaundice and the delayed cord severance group from Bumi Sehat enjoyed higher hemoglobin.
Our MotherBabies enjoy a breastfeeding rate of 100% upon discharge from all of our three Childbirth centers, in Indonesia and the Philippines. We attribute the success of Mother’s to breastfeed to the bright, enthusiastic way in which babies, born at our birth centers, bond wide-eyed, and go directly to the breast to self-attach and feed. Also the support of our midwifery team, for each MotherBaby, protects breastfeeding start-up. There is absolutely NO infant formula supplied or promoted at Bumi Sehat.
Babies who are compromised by newborn anemia, caused by the immediate or early clamping and cutting of their umbilical cords, are withered in comparison, and have more difficulty finding the energy required to self-attach and robustly feed at Mother’s breasts. After all, babies who suffer the routine medical habit of immediate cord severance, only seconds after birth, have been denied up to 1/3 of their divine right to their natural blood supply and stem cells, of course they have trouble breastfeeding. Sever anemia makes any and all newborn activities; gazing, crawling toward the breast, nuzzling, staying awake, latching and suckling, nearly impossible. I sing praises to the determined mothers who manage to bond and breastfeed their infants, in spite of immediate cord severance. Humans are super resilient, but that is no excuse to abuse them at birth.
No other Mammal, except humans, routinely interferes with bonding and breastfeeding by quickly severing the umbilical cords of their offspring.
No matter if you are rich or poor; educated or not; brown, black, white, red, yellow or of mixed race, Muslim, Christian, Buddhist, Hindu, Pagan, Catholic, Jewish or Agnostic, very young or getting older, if you go to a medical institution for childbirth, your baby will be robbed of up to 1/3 or 33% of his or her natural blood supply.
Why? Stem cells are valuable, blood is valuable, some hospitals sell babies’ blood for transfusions and for research. Many parents are asked to donate their babies cord blood to science or to help others. Is this blood not meant to help the baby it belongs to? If adults may only donate up to 10% of their blood, why are doctors taking up to 33% of our babies’ blood, without consent. There are hospitals and clinics who impede the natural transfer of blood from placenta to baby, only to throw it away as medical waste. Umbilical cords are marketed for transplants. Placentas have been sold to cosmetic companies to be used in beauty supplies.
Just say “NO, I will not allow anyone to abuse my newborn by immediately clamping and cutting my Baby’s umbilical cord!”
If you were born in a hospital or clinic, it happened to you. If you plan to have your birth in nearly any medical institution on earth, it will happen to your baby, unless YOU stop it. Immediate or early clamping and cutting of babies’ umbilical cords is the biggest most widespread, medically sanctioned Human Rights issue on Earth!
Join us for Eat Pray Doula: A Gentle Birth Workshop where you will visit Bumi Sehat Clinic, connect with other BirthKeepers from around the world, and learn from Ibu Robin and Debra Pascali-Bonaro.

Ibu Robin Lim is an internationally-recognized midwife, well-known author and talented poet. She was awarded the 2011 CNN Hero of the Year Award, and was nominated for the 2016 CNN Superhero award. Her non-profit Indonesian birthing and educational clinics Bumi Sehat have saved hundreds of lives and delivered thousands of babies over the last decade, serving the poor and medically disenfranchised citizens of Bali and, far away, in the tsunami-ravaged province of Aceh, Sumatra. After years of service and frequent financial challenges, “Ibu” (Mother) Robin and her organization remain indefatigably committed to changing the world, one gentle birth at a time. Please consider supporting Ibu Robin and her clinic by donating to Bumi Sehat Foundation, or adding Bumi Sehat Foundation International Inc as your Amazon Project SMILE link. (shop from http://smile.amazon.com and Amazon will donate t the charity of your choice.)